

I'm only going to respond when I can detect humanity — when I can detect a human being or signs of human life. 'Mural,' by Jackson Pollock. Inset of photo by Andy Rain. [o]
WHITNEY SMITH You are involved in an organization, the National Empowerment Center, whose mission is “to carry a message of recovery, empowerment, hope and healing to people with lived experience with mental health issues, trauma, and extreme states” — a noble but weighty mission if ever there was one. The main tool of this organization is something you and colleagues came up with, Emotional CPR, a kind of emotional distress approach. Similar in principle to the CPR we’re familiar with, cardiopulmonary resuscitation, Emotional CPR focuses on assisting people who are experiencing severe emotional distress. This strikes me as a significantly useful tool in a world where everyone, at some time in their lives, will have the opportunity to help someone in a drastic mental or emotional state — or maybe be in crisis ourselves and helped by someone else.
Before we get to how Emotional CPR (eCPR) works and the incident that inspired you to create it, tell me about who Daniel Fisher was before that time.
DANIEL FISHER Emotional CPR came from my personal experience, and I can pinpoint exactly when it happened, but before I do that I’ll lay out some useful context. My father was a doctor, a general practitioner and an internist who had a lot of things going on in his career. I greatly admired and respected him, and I worked in his lab when I was in high school. Coming from a family of many doctors, I wanted to be one, too, but I had a driving reason to be a doctor. As a teenager I had a burning question about what was wrong with my sister, who suffered from anorexia at an early age. Though she saw a child therapist, my father always believed it was due to a chemical imbalance. So this idea of biochemistry and its significant effect on our understanding mental health was foundational for me. Plus, when I was considering what to study in college, a friend of my father, who was head of research at our National Institute of Mental Health suggested biochemistry. So, while I was a hippie very involved in counter-culture politics of the Left in the 1960s, I got a PhD in biochemistry, in three years.
My answer was, "People that had less training seemed to express more of their humanity."
SMITH Early in your training in medicine you had an episode that revealed what was to become a founding principle of eCPR.
FISHER The moment of inspiration for eCPR came when I was in a mental state referred to as catatonia. I was not speaking, no words. I'm wheeled into the emergency room of Bethesda Naval Hospital, because my work was associated with this hospital, by two hippie friends — all three of us were obvious counter-culture, anti-war hippie types. When my friends realized they were in a military emergency room, afraid they might be kept there, they put me in a wheel chair and took off. I had no identification.
Someone came by with their clipboard and started asking me questions — what’s your name, address, name, social security number, who, where, why. I wouldn't even shake my head. Not knowing what to make of me, they just pushed me over to the side. They thought I was unreachable, at least that was how they behaved. I still wouldn't talk. This was not really voluntary on my part. Yes, I was thinking, but they were like very long thoughts. The main long thought I had was, if someone else had been where I am, they'd know how to be with me so I could communicate with them. That was a helpful thought. It was helpful because of all these people who came to me and tried to connect with me, I could identify the ones on the staff I could communicate with. That was thought number one. The second thought I had was, I'm only going to respond when I can detect humanity — when I can detect a human being or signs of human life.
I had become convinced that most people were on a kind of automatic pilot and had lost their humanity. I didn't want to communicate with people who had lost their humanity. How could I detect that they had lost their humanity? I didn't think it at the time — this was reconstructed later — but one of my answers to this question was: people that had less training seemed to express more of their humanity.
Time goes on. I’m in the wheelchair off to the side in the emergency room. In this military hospital there were people roaming about called corpsmen, 18 and 19-year-olds who had minimal medical training, very minimal. There were also psychiatrists, psychologists, psychiatric nurses — all the usual identifiable professionals — who I could have cared less about. In them I didn't detect the level of humanity I felt was necessary for me to respond. Putting such a value on my surroundings — only responding to those who show their humanity — was a rather harsh requirement. Then, it might have been five minutes or half an hour, I don't know, a corpsman sits down in front of me and looks into my eyes. He introduces himself, which nobody had done so far, and says, “Hi, I'm Rick.” I thought, that’s a good start. Rick says, “If you can hear me, can you nod?” He didn't even know if I could hear at that point. I nodded. Okay, he thinks, this guy can hear and respond. Given these facts, it is determined that I belong in the psych unit.
Once I was up there, I closed right back off again. But two corpsmen, John and Tori (interesting that I still remember their names), did what Rick had done. These three instinctively and intuitively knew how to reach me. Again, no real training and therefore, interestingly, open to whatever possibilities presented themselves, as opposed to, what did they teach us in medical school about this. It was as if they entered into a state of play with me — how about we try this? They used hand gestures — are you thirsty, are you tired — and other very basic things like that, which was terrific. They carried on with me in this way because, hey, it was working. It was also vital that they showed compassion and caring for my welfare. Once they did that, I began to interact. Without my words, we began conversing non-verbally. After about three weeks I started talking and a week later I was more or less back in shared reality. Then they determined they could let me go to my laboratory, which ironically was right across the highway from the hospital. I got to the lab and my lab technician, a wonderful guy, said, “Seeing you is like a ray of sunshine.” I was very touched.
When I returned to the psychiatric hospital however, problems developed. The staff asked me how I was feeling. On a scale of one to 10, I said 11. They decided I was too high and “escorted” me to seclusion where they forcibly injected me with a major tranquilizer. Just before I blacked out, I vowed to become a psychiatrist and not allow such treatment to continue. Soon after I visualized that I was a blue bird flying out the grated window to freedom where they could never capture my soul.

What is it we derive in connecting powerfully with others? Photograph by Leonard Freed, Dr. Martin Luther King, Jr. being greeted on his return to the US after receiving the Nobel Peace Prize, 1964. Courtesy of Magnum Photos.
Fast forward . . . I went to medical school, got through it, God knows how. But all through that time I kept thinking about what I had learned in that hospital stay. During my medical training, I couldn't stand up say to them, “By the way, I know how to reach people because I've actually been in catatonia.” They’d have said, “If the person is not talking, how in hell do you think you can communicate with them?” But as time went on, they saw that I actually could reach people — and they were shocked. Again, their training had not taught them how to reach an apparent ‘unreachable.’ I kept thinking, if only I could teach this.
LIFE IN THE PSYCHIATRY LANE
After I graduated my residency in 1979 and was doing all kinds of psychiatry, advocacy and self-help, I still hadn't figured out how am I going to teach this. Then in 2008, I learned about Mental Health First Aid. I thought, oh, that's a good idea. That must be for the public, because I want to teach everybody how to reach people in distress. Unfortunately, Mental Health First Aid was terrible. It basically teaches the lay public how to diagnose your out of sorts neighbour and turn them over to the authorities. I see. Well, I was shocked, and the whole advocacy movement I was involved with, was shocked. So what do you do? You can either fight things or you can create alternatives. So we created something, which was the start of this alternative, Emotional CPR. That was 2009 and we've been at it for 17 years now.
SMITH And what's the general method or principle of eCPR?
FISHER We started with the question I was asking when I was in catatonia: What did I most want when I was in the most distress? How did I want people to be? I wanted them to be human. A reasonable request, sure, but the problem is, what does it mean to be human? How do you do that, how do you be human? That’s the first question from which some conclusions can emerge. A second question is, who are we talking to — who are we forming this approach for? In our movement specifically, we mean people who have had a big time diagnosis, their life has been interrupted by some serious mental turmoil, or they had psychosis and or some other disorder that has made it very difficult to lead their life. So, that was our first target, how to help people in that state of existence — how to assist people through emotional distress, which is part of the mission I mentioned earlier.
THE SEVEN INTENTIONS OF EMOTIONAL CPR
SMITH Let’s say I’ve heard about your group and I’m interested. Perhaps I’ve had people in my life who I’ve been in contact who I’m at a loss to help when they become very distressed. How do I learn Emotional CPR?
FISHER The introduction to the approach lasts two days, and in that time we boil it down to what we call the Seven Intentions. Not rules, not even principles or a theory, just intentions. And I will say at the outset, although we developed eCPR for people in emotional crisis, we increasingly find it helpful in every communication. It becomes more like a way of being. And when I say that, I mean a way of interacting and communicating with others. Since we are all doing a lot of that in our lives, when we shift our approach to being with others in a manner different than usual, we discover some new things about how we are connecting with others.
SMITH So at the core, speaking broadly, would you say you are teaching communication skills?
FISHER To a degree, yes. Communication skills that get us out of the head and into the feeling realm. This discovery of being with others often happens when we lean towards helping somebody, as opposed to judging or arguing against what is going on with them. The First Intention is to communicate not just with our eyes and ears, but with our heart. We open our heart to the other person, and we're trying to communicate at the heart-to-heart level. So, rather than probing to determine a diagnosis, we first try to get in tune with the person. Be present with them and what it is they’re experiencing, without necessarily understanding it.

The Chinese character for listening . . . Tīng is all of them together. [o]
SMITH What I hear you saying is, when I listen with my heart I am listening with feelings rather thoughts, logic and reasonability (which is something I heard often in shamanic medicine courses, which my Western mind-position railed against). As opposed to, this person is in crisis and I'm suddenly here on the scene as an agent of aid needing success as a good person who plucks them from danger. Rather than: open the heart, listen with the heart, stop trying to be an achiever.
FISHER Yes, that's a good place to start. The Chinese word for listen — tīng — comes close to what you’re saying and what we’re intending with that intention. When I was teaching this course in Singapore and explained the first intention, people said, “Oh, doctor, you're talking about tīng — which is Chinese for listening with your eyes, ears and heart with full attention. And regard the other person as if they were an emperor. The Chinese character is a complex one: there is a character for the ear, a character for the eye, a character for the heart. Tīng is all of them together.
The Second Intention is: I will experience certain feelings being with you, certain sensations, and I will make space for those feelings and sensations. A common response is to use emotional expression to maintain boundaries, which we want to avoid doing. The idea is not only for me to be aware of my responses to what’s going on with the other person, but also to know that I do not have to respond immediately. That a neutral response can be a positive action.
SMITH What is propelling this approach?
FISHER There are various reasons. We’re trying to break the cycle of overly immediate and reflexive responses. We emphasize resonating rather than reacting. My first reaction in being with a person in distress might be, “You make me sad,” or, “you make me angry.” Instead of stating these feelings right away, as a reaction to the person in distress, we allow ourselves to sit with the first feelings, allowing ourselves to resonate with our deeper unique feelings which prepare us for our third intention. We're trying to help the other person to experience a variety of feelings that they may well may be having, but are not aware of. And so, we are like a resonating filament for their feelings that this other person is not yet aware of.
SMITH A resonating filament, that’s nice. Or a tuning fork.
FISHER Yes.
SMITH On a piano, when we hit a low note and push the sustain pedal down, which allows all the other strings to vibrate freely, the upper strings respond sympathetically with that one note — and one of the results of this is chords and scales. Tell me if this makes sense. In the situation of a person in emotional distress, is it as if they are the low note and we allow ourselves to respond to them sympathetically, rather going against what’s happening with them, or intervening or interrupting their state of distress?
FISHER Yes, we use the term “we are resonating” to indicate that we are allowing our deeper feelings to be experienced. In so doing we are role modelling so that the person in distress can expand the spectrum and the depth of their feelings.
The healing occurs in relationship, the two of us together. Not: "I am the expert who relieves the symptoms of the person who is labelled ill."
SMITH As you’ve said in many ways already, doing things, such role modelling, that are non-verbal and expressive of the ‘vibe’ you’re putting out, which grows from this heart-oriented stance.
FISHER Exactly. With the Third Intention, it is this: I will share the deeper, dynamic feelings that I am experiencing, which may or may not be their feelings. By sharing my feelings with the other person, it can open the channel for them to start experiencing the flow of their feelings.
SMITH So is it when they experience me feeling something — as opposed to me telling them something — this registers with them by cutting through the barrier they have by being **told things and, in some ways, patronized?
FISHER Yes, and it seems they often need permission to feel. I think in our western culture we all have a barrier to experiencing process of our feelings in depth. But when I can experience and express my feelings, it seems to lift the barrier to the feelings of the person in distress. In most situations we experience distress more from our being stuck in our heads as we suppress our deeper feelings than being distressed by the feelings themselves. We might only be aware of the anxiety and fear of the deeper feelings of despair and sadness, not of the sadness and despair themselves.
The Fourth Intention is: I will be with you. I will not do, just as you were saying. I will not explain, I will not fix, judge or advise you on what you're going through. And, I am not the expert that has the power to heal the broken person. I will just be with you.
SMITH Is this notion of “I am the expert who has the power to heal the broken person” embedded in the culture of the physician?
FISHER Yes. I conclude that the view that physicians have the power to heal the broken person is embedded in our Western culture, and I believed that when I first entered psychoanalysis. After two months of daily therapy I asked my analyst to tell me what was wrong with me and what treatment plan did he propose to cure me. His response was, "What is this need you have for me to heal you?" To which I replied that he was the doctor and expected he would heal me. He said, "But you are a doctor, too." His response I believe was helpful to my gradual realization that, contrary to popular belief, the power to heal lay inside of me, not him.
SMITH. I now see more clearly what you've been up against in developing eCPR. Not surprising, since during your catatonia crisis at the naval hospital you discovered that those with very minimal medical training were the most help to you.
FISHER Yes. The Fifth Intention is: Since I am not sure what is best for you, we will explore the unknown together. Our first version of this intention was: We will accept the unknown, or, we will accept uncertainty. But that’s too frightening for people — to accept the unknown. Rather than that, you do this, it’s more like: We will explore the unknown. Come with me, let’s look around together. You may notice that in this fifth intention we introduce the idea that we are in this together. This is crucial because it helps the person to realize they are no longer alone.
SMITH Mystery loves company.
FISHER Yes! And, it’s a little bit like that great Ionesco quote, “Explanation separates us from astonishment, which is the only gateway to the incomprehensible.” When you allow astonishment, you are given a pass into mystery.
Vincent Van Gogh, Self-Portrait with Bandaged Ear. (1889)
SMITH That which we don't know is engaging and interesting . . .
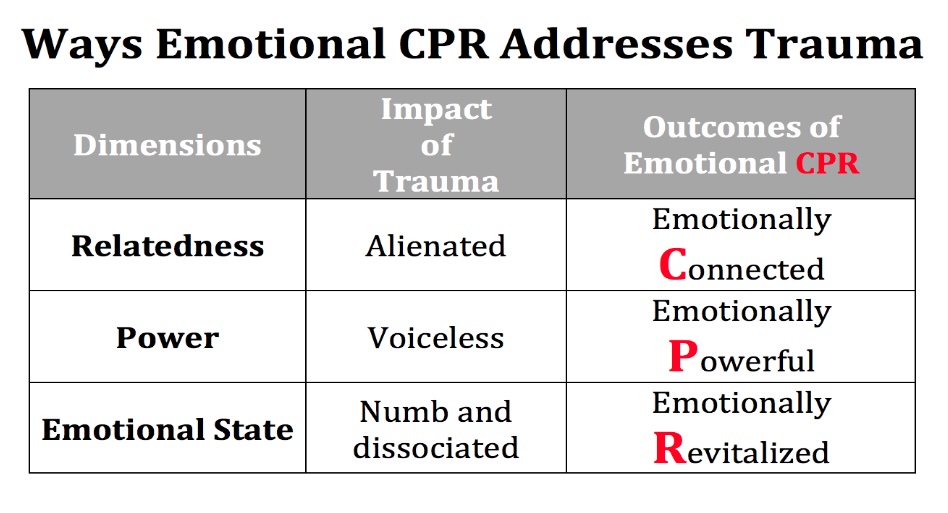
FISHER . . . and vitalizing, right? Actually, in the letters CPR, in our version of CPR the C stands for connect, P is for empower (we cheated a bit), and R is for revitalization. Emotional CPR is about bringing people back to life. Through Emotional CPR, we help people to experience revitalization and bring them back in touch with their humanity.
The Sixth Intention is: We have the power in us to heal. The healing we’re speaking of here occurs in relationship, the two of us together. Not, "I am the expert who relieves the symptoms of the person who is labelled ill." Also, not: You have the power within you, so good luck — just go out and do it, bye-bye!
SMITH Brutal, and lack of being presence with the other.
FISHER Yes. The Seventh Intention is: we create new life, new voice, and new hope in the present moment which is revitalizing. This new life comes from the freeing of our emotions which are an essential component of our feeling alive. When we can experience our feelings and express them, we are also accessing the energy that was being expended in suppressing those feelings before eCPR.
SMITH And what kind of response do you receive from sharing CPR?
FISHER We’re doing this all over the world. I have done about 150 of them myself, and we’re getting many responses. I remember one woman spoke of feeling like she’d had a transfusion. Others will say, I really came alive. I didn't realize I was asleep. I feel my feelings more.
SMITH I’m not dismissing what you’ve just said, but these are the kinds of responses are common to many, for lack of a better term, rejuvenation workshops. But what I think is new about what you’ve presented is that this is a language and method for emotional violence and distress that is both portable and easily learnable. For instance, a grand idea, if all young people came into the world as adults having learned these skills, it seems we’d all be in a much more peaceful place. And, by all of us helping those who who are burdened by a lot of very difficult things, emotional, psychological, biochemical, and so on. All the pain out there in the world.
FISHER That is what we’re trying to do, by taking it to a broader scale. It's mutual aid, really. Mutuality. We teach this across many cultures, and it crosses cultures very well. And when we do it in another culture we find that doing it in the native language rather that English is best. For instance, in Iceland, I was fooled into thinking they were getting it just fine in English — partly because many of them speak English very well there. But I noticed that when they were interacting at break, in the mother tongue they grew up with, they were much more animated, more free to express their feelings. I find that most bilingual people have a deeper learning experience in their mother tongue.
Courtesy of the Naitonal Empowerment Center.
SMITH What are the obstacles for bringing eCPR to scale?
FISHER One obstacle is the dimension of the Western culture of fixing, which I partly addressed earlier when you asked by As in: I’m in a situation where I think I can help you by getting you to do something, or I do something for you or to you. This is against the idea that the power is in the person themselves. I've got the power, and I might give some of it to you. That is not the way to bring people’s vitality out. That is about getting them to comply, getting them to behave themselves. In my part of the world, we’ve changed the term mental health here to behavioral health. I've said to people, you should just call it behave-yourself health! Going back to my earlier story about being in catatonia, the conventional mental health world is against the value of our finding where is the humanity in me? We need to find the humanity in our self in order to be human with the person who is himself in need of an authentic connection with another human being.
SMITH How can this sustain itself and grow — both financially and through its reputation?
FISHER We have departments of mental health, like in Los Angeles County, that contract us for eight to ten trainings every year. It's now become so popular there that now they expect that all their direct care workers will learn it.
SMITH What do you hope to see happen with eCPR?
FISHER My dream is that the whole world will do it. It’s like CPR that saves people by helping them get through a heart attack. I dream of a world where everyone will become conversant in eCPR, and where, in so doing, the incidence of major mental illness will go down. It's a primary prevention not just for major mental illness, but for life distress as well. That's one dimension of it. Another is that generally speaking, what you said, there’ll be more peace in the world because people will be able to communicate better with each other. ≈ç
CODA: ON DIAGNOSING SCHIZOPHRENIA
SMITH You spoke earlier of being diagnosed with schizophrenia at the naval hospital during your catatonia episode. Given that you have degrees in biochemistry and psychiatry, and have created this approach for people suffering from emotional distress, I'm interested in what you have to say about your diagnosis of schizophrenia and schizophrenia diagnoses in general, which has always been controversial to various degrees.
FISHER I think the diagnosis of schizophrenia is more damaging than helpful. I think the US should follow the example of three Asian countries (Japan, Taiwan and South Korea) and Hong Kong and drop the diagnosis from our DSM (The Diagnostic and Statistical Manual of Mental Disorders). My reasons for eliminating the diagnosis of schizophrenia are:
1 There are no objective criteria for the diagnosis. There is no chemical blood test or reliable biological or genetic defect characteristic of schizophrenia. Even the former director of the NIMH, Dr. Thomas Insel (who was director for 13 years) stated that after spending 20 billion dollars on research they were unable to find a specific biological basis of any psychiatric diagnosis, including schizophrenia. Drs. Rudolph Uher and Michael Rutter concluded that there has been no consistent genetic basis found for any psychiatric disorder.
2 We can not reverse the greater than 100 year history of the diagnosis: Ever since Emil Kraepelin described the condition dementia praecox, (in 1899) which was later called schizophrenia, there has been a false belief that people never recovered from that condition. Kraepelin and Bleuler suffered from what Dr. Courtnay Harding has called the clinician's delusion. Both these early psychiatrists only saw patients in their psychiatric hospitals. In their era very few patients ever left the hospital because of institutionalization and a lack of hope by all involved. In fact even in their era the recovery rate for persons receiving moral therapy was greater than 50%, but they were never seen in follow up by the two inpatient psychiatrists. Eugen Bleuler's own son, Dr. Manfred Bleuler carried out followup studies of patients discharged from the same hospital as his father had worked. The son found that the recovery rate was much higher than the father ever observed. More recent studies by Dr. Harding and many other epidemiologists have shown that given robust, hopeful community supports a majority of persons diagnosed with schizophrenia recover a full and meaningful life in the community.
The conviction that schizophrenia is a permanent condition from which people do not recover remains today, even in higher level graduate courses on abnormal psychology. The professor of a friend of mine lectured that people do not recover from schizophrenia. She told the professor that a friend of hers, me, had recovered from schizophrenia. He said the friend must have been misdiagnosed. So my friend and I went over the criteria of schizophrenia in the DSM 4; I had met all the criteria for the diagnosis. When she repeated this finding to her professor, he said, “Well, then we have a case of a disabled psychiatrist."
3 Anyone, given sufficient stressors and isolation from social supports can exhibit symptoms of psychosis: A dramatic example is that over 90% of persons who traumatically lose vision in both eyes can become psychotic. This is the reason that eye surgery is only done on one eye at a time. When I treat a patient who has been given a diagnosis of schizophrenia I explain all these problems with the diagnosis, as well as tell them I myself had received such a diagnosis. I describe to them that I was able to recover. I then emphasize that many people can and do recover and that we will work towards that goal.
RELATED TO THIS INTERVIEW
• National Empowerment Center, co-founded by Daniel Fisher
• Emotional CPR: Assisting People Through Emotional Distress
Editors: Barbara Meyers, Daniel Fisher, W. Reid Smithdeal, Oryx Cohen, Shira Collings
92 pp. Published in 2024.
• Heartbeats of Hope: The Empowerment Way to Recover Your Life
By Daniel Fisher
272 pp. Published in 2017.

DANIEL FISHER is a psychiatrist, researcher and mental health recovery advocate and educator. He developed the Empowerment Model of Recovery and the PACE/Recovery program to shift the system to a recovery orientation. From 2002-2003 he was a Commissioner of the President’s New Freedom Commission on Mental Health. Well recognized in his field, he has received the Clifford Beers National Mental Health Association Award and the Bazelon Center for Mental Health Law’s Advocacy Award. He lives in Cambridge, Massachusetts.
Add new comment